If you are researching the ALF (Advanced Lightwire Functional) appliance for your child, you are doing exactly what a thoughtful parent should do — looking into the details before committing to treatment. This article is here to give you the clinical perspective that ALF marketing materials do not.
The ALF appliance is positioned as a gentle, holistic approach to jaw expansion. Providers often describe it as a way to achieve:
✅ Jaw expansion without forceful pressure
✅ Tongue positioning and myofunctional training
✅ Airway improvement and better nasal breathing
✅ Avoiding traditional palatal expanders
These are worthy goals. We share many of them with our whole health approach. But after years of treating patients who come to us during or after ALF treatment, we have seen a consistent pattern: the ALF appliance frequently does not deliver true skeletal expansion. Instead, it tips teeth outward — creating the appearance of a wider arch while leaving the underlying jaw width unchanged.
This is not a subtle distinction. When teeth are pushed outside their supporting bone without the jaw itself widening, the consequences can include gum recession, bite instability, jaw joint pain, and the need for additional treatment to correct what the ALF was supposed to fix. Many of the patients we see after ALF treatment tell us the same thing: they wish someone had explained this difference before they started.
We want you to have that information now — before you make a decision.
What We’ve Seen in Our Practice After ALF Treatment
Over the years, we have treated numerous patients who came to us after using the ALF appliance — sometimes for several years — without achieving the results they were promised. While every case is different, the patterns are remarkably consistent. Understanding the difference between skeletal expansion and dental flaring is essential, and these cases illustrate why.
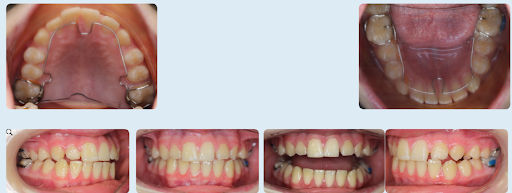
Case 1: 12-Year-Old Boy After ALF Treatment
This patient had used the ALF appliance for multiple years. When he arrived at our office, he was frustrated with the appearance of his teeth — feeling they stuck out too far. He experienced discomfort when chewing and a persistent feeling that his bite was off. His family sought a second opinion because the treatment they had invested years in did not seem to be working.
Here is what our evaluation found:
This patient had used the ALF appliance for multiple years. However, when he arrived at our office, he was frustrated with the appearance of his teeth, feeling they stuck out too far. He also experienced discomfort when chewing and a general feeling that his bite was off, prompting him to seek a second opinion.
Here is what our evaluation found:
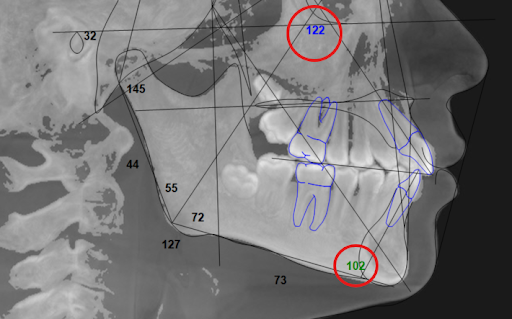
Flared front teeth
The boy’s incisors had been pushed forward, creating the appearance of expansion when in reality his teeth were simply tipped outward. (Exhibit A: Any number that is not black is out of the norm. In this case both the upper and lower incisors were out of the norm because they were both flared out considerably.)
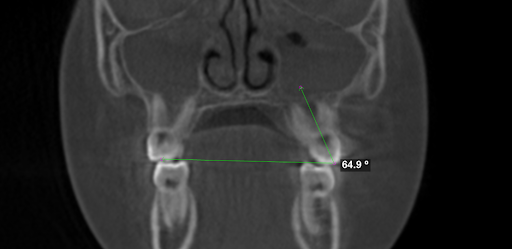
Severely tipped out teeth
His molars were leaning outward at a 65-degree angle, when we ideally want them closer to 90 degrees for proper stability and interdigitation of the upper and lower teeth.
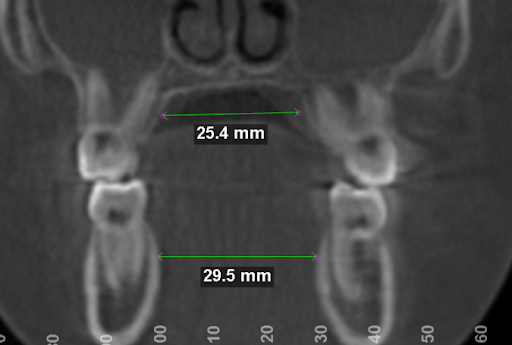
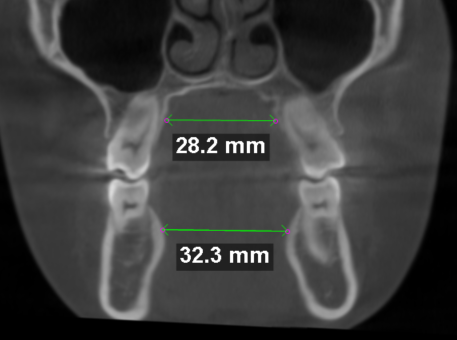
No true skeletal expansion
When we measured his upper and lower jaw widths using our 3D CBCT scan, we found that his upper jaw was still too narrow in relation to his lower jaw. The ALF had not created real orthopedic change, despite years of use.
Our evaluation of this case used advanced 3D CBCT imaging — not just visual assessment or flat panoramic X-rays. These traditional methods do not show the full scope of what is happening structurally. 3D imaging combined with the clinical experience to interpret it is essential for accurately diagnosing what ALF treatment has or has not accomplished.
Case 2: 15-Year-Old Girl with TMJ Pain After ALF
This patient had previously undergone ALF treatment and Invisalign with another provider. By the time she reached our office, she was experiencing severe TMJ pain — constant, debilitating jaw pain when chewing or opening her mouth wide, clicking and popping in her jaw joint, and a bite that felt uneven and uncomfortable. After years of orthodontic treatment, she was dealing with problems that should not have been there.
Her family came to us because they needed answers. Here is what we found:

Tipped molars and an unstable bite
Her upper molars had tipped outward due to ALF, disrupting the balance of her bite and creating the instability that was directly contributing to her pain.
Skeletal discrepancy remained
Her 3D scan confirmed that, despite ALF use, her upper jaw had not expanded sufficiently to match her lower jaw. The fundamental problem was unchanged.
TMJ dysfunction
The instability in her bite was a major contributing factor to her jaw pain — a problem that could have been prevented with proper orthopedic expansion from the beginning.
These are not isolated cases. They represent a pattern we see regularly: the ALF appliance moves teeth without moving bone, and the patient is left with instability, discomfort, and the need for further treatment.
If any of this sounds familiar — if your child has had ALF treatment and you are seeing teeth that stick out, a bite that does not feel right, or jaw pain that was not there before — we offer complimentary second-opinion consultations. A 3D CBCT scan can show you exactly what has happened structurally and what it will take to correct it. Schedule a second-opinion consultation with Dr. Chantal Hakim.
What About Biobloc Orthotropics?
Another approach sometimes considered under the umbrella of holistic orthodontics is Biobloc Orthotropics. Like the ALF appliance, Biobloc aims to guide jaw growth, improve breathing, and support facial balance using removable appliances adjusted over time.
We have seen similar patterns in patients who come to us after Biobloc treatment. Teeth tipped outward rather than true jaw expansion. Bites that are unstable. The same fundamental question applies: is the treatment actually changing the bone, or is it only moving teeth?
When the bone is not truly expanding, the same problems arise — instability, jaw pain, and teeth that do not line up correctly. The goals of these approaches are understandable, and we share the commitment to supporting natural growth and whole-health outcomes. But the method must produce measurable skeletal change, not just dental movement that will not last.
Why True Skeletal Expansion Matters
When the upper and lower jaws do not align in width — what orthodontists call a transverse discrepancy — the solution is to widen the jaw itself by growing new bone. Not tilting teeth. Not flaring arches. Actual skeletal change.
This matters for reasons that go well beyond straight teeth:
Airway and Breathing
The roof of the mouth is also the floor of the nose — and expanding the palate directly improves the nasal airway. When the upper jaw is expanded at the skeletal level, the nasal airway widens with it. This can improve nasal breathing, reduce mouth breathing, and support healthier sleep — outcomes that affect a child’s development, focus, and daily quality of life.
Tongue Space and Oral Function
A properly developed upper jaw gives the tongue room to rest in its natural position against the palate. This influences breathing, swallowing, speech, and even facial growth patterns over time.
Long-Term Stability and Tissue Health
When expansion is achieved by flaring teeth outward without skeletal change — as we frequently see after ALF treatment — the teeth can be pushed beyond the boundary of their supporting bone. This leads to gum recession, root exposure, bite instability, and results that do not hold. True skeletal expansion builds new bone, creating a foundation that is stable and lasting.
If you are currently evaluating treatment options for your child and want to understand whether true skeletal expansion is what they need, we can help you find out. A complimentary consultation includes 3D imaging that shows the jaw, the bone, and the airway — so the conversation starts with objective evidence, not assumptions. Schedule a consultation with Dr. Chantal Hakim.
How Dr. Chantal Hakim Ensures True Skeletal Expansion
The difference between what we do and what ALF claims to do comes down to three things: how we diagnose, what appliances we use, and what we measure along the way.
Objective 3D CBCT Analysis
We do not rely on visual assessment alone. Our practice uses 3D CBCT imaging to accurately and objectively measure the width of both the upper and lower jaw. This allows us to determine whether expansion is actually needed rather than assuming, measure exactly how much expansion is required — we typically aim for the upper jaw to be 2mm wider than the lower jaw to ensure a proper skeletal relationship, and confirm throughout treatment that true skeletal expansion is taking place rather than dental tipping.
Precision-Oriented Appliances
Instead of relying on light forces to nudge teeth outward, we use scientifically validated orthopedic appliances that directly stimulate bone growth. The expansion is gentle — but it is measurable, skeletal, and stable.
A Whole-Health Evaluation
Jaw width is one part of the picture. We evaluate sleep and breathing patterns, jaw joint health, facial growth trajectory, and how all of these factors connect. Both Dr. Chantal Hakim and Dr. Isaac Hakim are board-certified orthodontists trained in the Roth Williams philosophy of functional occlusion — a clinical framework that starts with the position of the jaw joints and builds the treatment plan from there. This is how we ensure expansion is done correctly the first time — treating the whole child, not just shifting teeth into a position that looks acceptable temporarily.
What Patients Tell Us They Wish They Had Known
The families who come to us after ALF treatment are not careless. They are parents who researched their options, chose what sounded like the gentlest approach, and trusted a provider who promised results. What they tell us, consistently, is that they wish they had understood three things before starting:
That there is a difference between moving teeth and moving bone. ALF marketing describes “expansion” without distinguishing between dental tipping and true skeletal change. These are fundamentally different outcomes, and the long-term consequences are very different.
That years of treatment without measurable progress is not normal. Several families we have worked with describe spending two, three, or more years in ALF treatment without objective evidence that the jaw was actually widening. In a properly planned expansion case, measurable skeletal change is visible on imaging within months, not years.
That the cost of correcting ALF problems is on top of what they already paid. This is the part that frustrates families the most. After investing significant time and money in ALF treatment, they are now facing additional treatment — and additional cost — to correct the problems that treatment created.
We share this not to alarm you, but because these are the things a parent deserves to know before choosing a treatment approach. If you are considering ALF for your child, ask the provider to show you objective 3D imaging evidence that the jaw bone itself is expanding. If they cannot, that is important information.
Take the Next Step
Whether you are researching ALF and want an objective clinical perspective, your child is currently in ALF treatment and you have concerns about the results, or your child has completed ALF treatment and is dealing with instability, discomfort, or jaw pain — a second-opinion consultation can give you the clarity you need.
At the Orthospaceship, that consultation includes 3D CBCT imaging that shows exactly what is happening with your child’s jaw, bone, bite, and airway. No guesswork. No assumptions. Just objective evidence and a clear explanation of what it means and what your options are.
Schedule a complimentary second-opinion consultation with Dr. Chantal Hakim to find out what is really going on — and what the right path forward looks like.